Want to learn more about surgical guide planning?
Discover how digital workflows can improve your implant success rates.
Table of Contents
Zygomatic implants represent one of the most demanding procedures in modern implantology. When a patient has severe maxillary bone loss — often after years of complete denture wear — conventional implants simply cannot be placed. There is not enough bone to anchor them.
Zygomatic implants solve this by anchoring into the zygomatic bone (the cheekbone), bypassing the atrophied maxilla entirely. But the surgical trajectory is extreme: implants measuring 30-55mm pass through or alongside the maxillary sinus, close to the orbit, and emerge through the alveolar ridge.
Without meticulous 3D planning, the risks are unacceptable.
Case Presentation
Patient: 58-year-old female with severe bilateral maxillary atrophy
History: Complete denture wear for 15+ years, progressive bone resorption
Chief complaint: Unstable denture, inability to eat normally, social embarrassment
Diagnostic Findings
analysis revealed:
- Residual ridge height of 2-4mm in the premolar regions
- Complete pneumatization of both maxillary sinuses
- Adequate zygomatic bone quality (Bedrossian Type 2)
- Sufficient anterior maxillary bone for 2 conventional implants
- No pathological findings in the proposed trajectory zones
Treatment Plan
After multidisciplinary consultation, a Quad-Zygoma approach was selected:
- 4 zygomatic implants (2 per side) — anchored into the zygomatic arch
- 2 conventional anterior implants — placed in the remaining anterior bone
- Total: 6-implant-supported fixed prosthesis with immediate loading
Digital Planning Workflow
Step 1: Prosthetic-Driven Design
The workflow began not with bone analysis, but with prosthetic planning. A digital wax-up defined ideal tooth positions, ensuring that implant emergence would support the final prosthetic design.
Step 2: Zygomatic Bone Segmentation
3D segmentation isolated the zygomatic bone from the surrounding anatomy, create a clear visual zone for trajectory planning. The maxillary sinuses were segmented separately to map their exact boundaries.
The process of separating bone, teeth, nerves, and sinuses in a CBCT scan into individual 3D structures. It enables precise anatomical visualization for treatment planning.
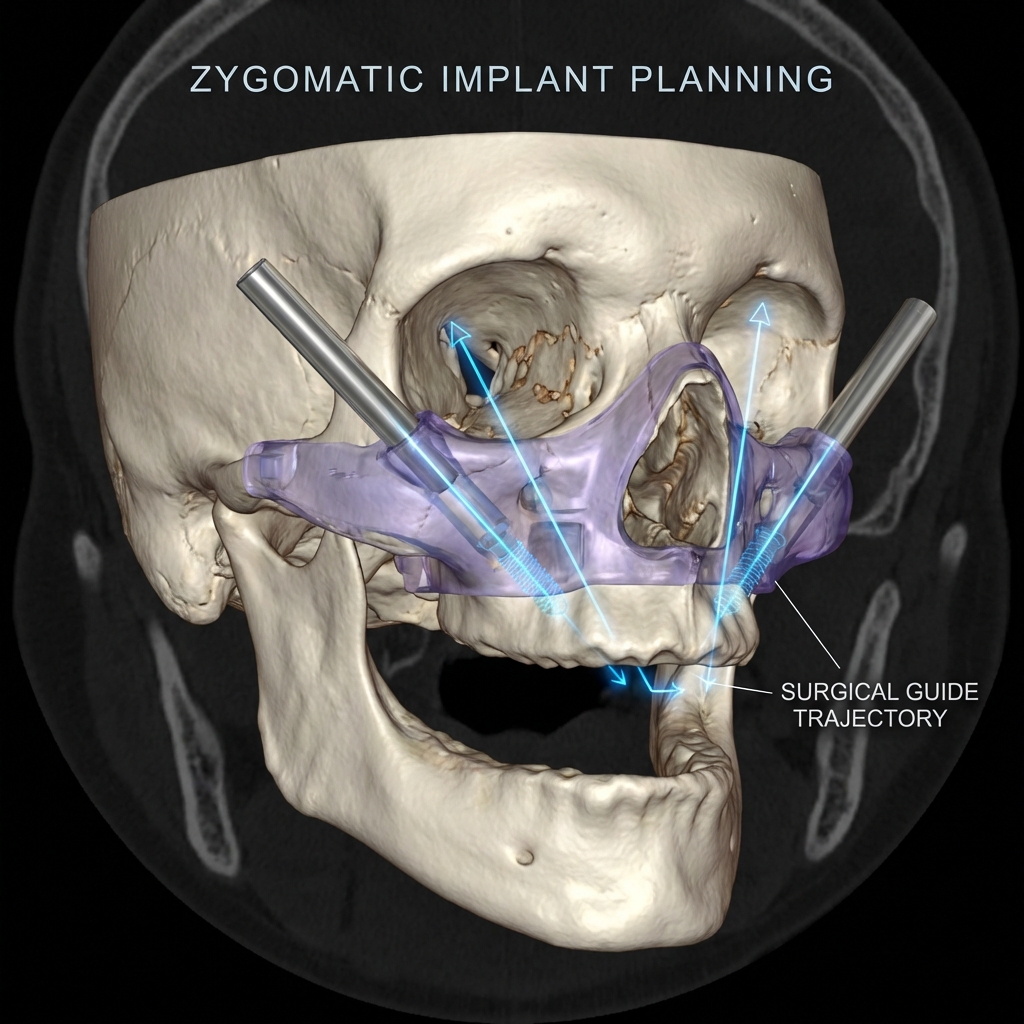
Step 3: Trajectory Planning
Each zygomatic implant was planned to:
- Avoid penetration of the orbital floor
- Minimize sinus membrane disruption
- Achieve palatal emergence (critical for prosthetic access)
- Maintain at least 2mm clearance from adjacent implants
Step 4: Guide Design
Given the complexity of simultaneous zygomatic and conventional implant placement, we designed a stackable guide system:
- Primary guide — bone-supported, for initial osteotomy and trajectory verification of all 6 implants
- Secondary guide — for final drilling and depth control
- 5 fixation pins — ensuring absolute stability during the extended surgical procedure
Step 5: Drilling Report
A detailed drilling protocol was generated specifying:
- Drill sequence for each implant position
- Recommended insertion torque values
- Sleeve specifications and drill kit compatibility
- Emergency contingency positions
Surgical Outcome
The procedure was performed under general anesthesia:
- All 6 implants achieved primary stability above 35 Ncm
- The patient received a provisional prosthesis the same day (immediate loading)
- Total surgical time: 3 hours 15 minutes
- At 6-month follow-up, all implants showed excellent osseointegration
- The patient reported dramatically improved quality of life
Key Takeaways
- Complex cases require thorough 3D planning — freehand zygomatic surgery carries unacceptable risk
- Stackable guides provide superior control for multi-phase procedures
- Prosthetic planning must precede implant planning — not the other way around
- Close surgeon-planner collaboration is essential for trajectory optimization
- Proper guide fixation is critical — zygomatic procedures involve significant drilling forces
FAQ
Can you plan zygomatic implants for any CBCT scan?
A 3D imaging technique that captures the jaw, teeth, and bone structure in a single rotational scan. It produces DICOM files used for implant planning, nerve mapping, and surgical guide design.
The CBCT must include the full zygomatic arch in the field of view. Small-field scans that capture only the alveolar ridge are insufficient.
How long does zygomatic case planning take?
Due to the complexity, zygomatic cases typically require 3-5 business days. We do not offer express delivery for zygomatic cases — accuracy takes priority.
Do you support extra-sinus (ZAGA) approaches?
Yes. We plan both intra-sinus and extra-sinus (ZAGA classification) trajectories based on the surgeon's preference and the anatomy.
---
Have a complex case to plan?
Upload your CBCT and describe the clinical scenario.
Ready to streamline your surgical guide workflow?
Join 200+ dental professionals who trust SurgicalGuide.Pro for precision planning.



